

ORIGINAL ARTICLES
Background. Despite declining stroke mortality in Eastern European countries, the burden of stroke measured as years lived with disability (YLD) has not shown a decreasing trend, giving rise to the so-called “rehabilitation paradox”.
Objective: To assess trends in the burden of stroke in Lithuania, Russia, Moldova, Estonia, and Czechia from 2010 to 2021, and to model neurorehabilitation needs and workforce shortages.
Material and methods. A secondary analysis of data from the Global Burden of Disease Study (GBD) 2021 was conducted. Both absolute YLD counts and YLD rates per 100,000 population were examined. The estimated annual percentage change (EAPC) for 2010–2021 was calculated. Based on GBD data, the demand for neurorehabilitation services was modeled and workforce shortages were estimated for the countries under analysis.
Results. In 2021, the highest YLD rates per 100,000 population were observed in Lithuania (333.3) and Russia (305.8). A decline in YLD was identified in Estonia (EAPC –0.9%; –9.7% from 2010 to 2021) and Czechia (EAPC –1.6%; –14.6% from 2010 to 2021). In Russia, the absolute YLD burden increased by 2.2% (up to 454.3 thousand individuals). The shortage of rehabilitation professionals was estimated at 14,855 in Russia, 366 in Moldova, and 282 in Lithuania. Sensitivity analysis for 2010–2019 confirmed the observed trends; the impact of COVID-19 was found to be moderate.
Conclusion. A rehabilitation gap persists across all five countries. Scaling up neurorehabilitation services in accordance with the standards of the European Stroke Organisation and the World Health Organization is required.
Background. Pre-rehabilitation improves surgical outcomes in cancer patients; however, its necessity for different stages of cervical cancer (CC) remains insufficiently justified. Thus, a comprehensive assessment of the preoperative status of patients is required.
Objective: To evaluate various quality of life (QoL) components and objective health indicators in CC patients prior to surgical intervention, thereby substantiating the necessity for pre-rehabilitation.
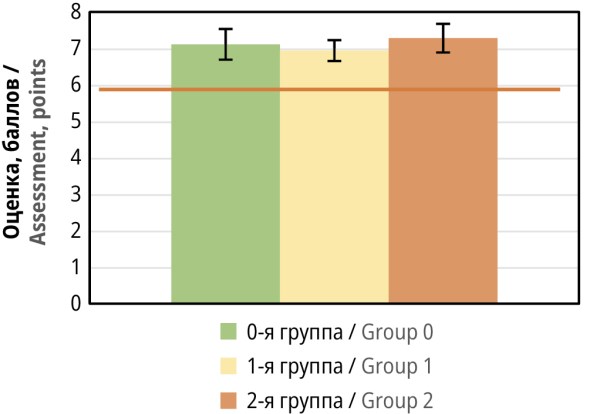
Material and methods. The single-point interventional study included 199 patients with verified cervical cancer in situ or stages I or II (Groups 0, 1, and 2, respectively). QoL was assessed using the Functional Assessment of Cancer Therapy – General/Cervix (FACT-G/Cx) questionnaire; distress level was evaluated using the adapted International Psycho-Oncology Society (IPOS) methodology. Body Mass Index (BMI), vaginal pH, human papillomavirus 16/18 viral load, blood levels of glucose, insulin, Homeostasis Model Assessment of Insulin Resistance (HOMA-IR) index, as well as leptin, tumor necrosis factor alpha (TNF-α), interleukin-6 (IL-6), and magnesium concentrations were determined.
Results. A significant decrease in QoL across all FACT-G/Cx domains was revealed, most pronounced in patients with stage II CC (total score 100 [95.5;104.0]). The IPOS distress level was ≥6 points in all groups. BMI ranged from pre-obesity (Group 0) to class I obesity (Groups 1 and 2). Insulin resistance was registered in all patients: HOMA-IR was 2.98±0.40 (Group 0), 4.09±0.81 (Group 1), and 5.34±0.80 (Group 2). Elevated TNF-α and IL-6 concentrations were observed in all groups, peaking in patients with stage II CC. Serum magnesium deficiency (<0.80 mmol/l) was present in all cases.
Conclusion. Prior to surgery and regardless of stage, CC patients experience a significant decrease in QoL, elevated levels of psychoemotional distress, overweight, insulin resistance, systemic inflammation, and magnesium deficiency. The severity of these impairments increases with more advanced stages of CC. These findings substantiate the need for the early initiation of multimodal pre-rehabilitation in the period from diagnosis until surgical intervention.
REVIEW ARTICLES

Background. Breast cancer-related lymphedema (BCRL) of the upper limb is one of the most frequent and disabling complications of treatment, having detrimental effects on the functional status, quality of life and social adaptation of such patients. Despite widespread use of non-pharmacological rehabilitation interventions, the issues of their comparative effectiveness, optimal combinations and long term outcomes continue to be debatable. An analysis of international guidelines in the context of Russian clinical experience is a relevant research task.
Objective: To carry out a systematic review of scientific publications on non-pharmacological rehabilitation methods for patients with BCRL of the upper limb.
Material and methods. The review was carried out according to the PRISMA 2020 guidelines. Literature search was conducted across the PubMed/MEDLINE, Scopus, Web of Science, Cochrane Library, PEDro and eLibrary databases and covered the period from 2000 to 2025. The analysis included clinical guidelines, systematic reviews and meta-analyses, randomized controlled trials and cohort clinical studies evaluating complete decongestive therapy (CDT), compression therapy, physical exercise, manual lymphatic drainage, kinesio taping, low level laser therapy (LLLT), intermittent pneumatic compression (IPC), instrumental physiotherapy and surgical methods. The risk of bias was assessed using Cochrane RoB 2, ROBINS I, and AMSTAR 2 tools.
Results. A total of 33 sources were included: clinical guidelines (n=3), systematic reviews and meta-analyses (n=10), randomized controlled trials (n=7), and cohort/prospective studies (n=3), as well as reviews, methodological and clinical works (n=10). CDT has the strongest evidence base and is considered the “gold standard” for BCRL management. Compression therapy is effective for both prevention and remedial treatment. Physical exercise is safe given proper compression and improves functional outcomes. Manual lymphatic drainage is considered effective as a component of CDT. LLLT, kinesio taping, and IPC have a moderate evidence base as adjunctive modalities. Russian studies highlight the potential of instrumental physiotherapy and surgical approaches, although requiring further validation in multicenter randomized controlled trials.
Conclusion. The effectiveness of a multicomponent rehabilitation strategy in BCRL of the upper limb has been confirmed. CDT remains the method of choice, while individualized programs incorporating physical exercise, instrumental techniques and surgical interventions extend treatment opportunities at different stages of the disease. Further multicenter studies are required to clarify optimal combinations, long term outcomes, and cost effectiveness of various approaches.
Background. Cerebral palsy (CP) is the leading cause of childhood disability with a prevalence of 2–3 cases per 1,000 live births. Traditional rehabilitation methods often fail to provide objective real-time feedback. Biofeedback (BF) technologies represent a promising approach that allows neuroplasticity to be activated through conscious control of physiological parameters.
Objactive: Critical review and synthesis of available evidence on the role and effectiveness of BF systems in comprehensive rehabilitation of CP patients.
Material and methods. A systematic search was conducted across PubMed/MEDLINE, Scopus, Web of Science, Cochrane Library, PEDro, Embase, CyberLeninka, and eLibrary databases. The search depth was from 1965 to November 2025. The inclusion criteria were: studies that employed BF technologies in CP patients and reported measurable motor outcomes. The quality of the conducted research was assessed using the PEDro, Downs and Black, SCED scales, as well as the Cochrane RoB 2 tool.
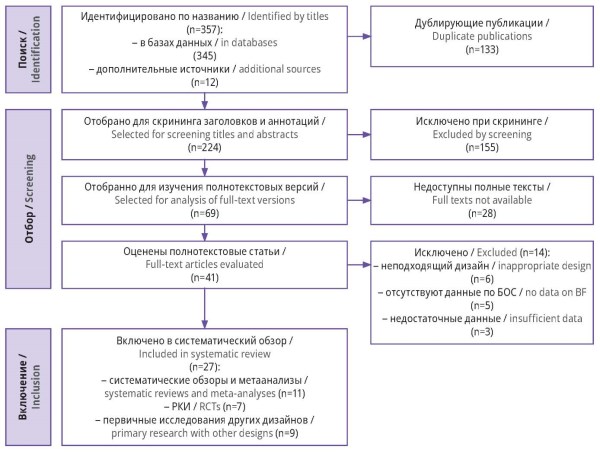
Results. In total, 27 publications were selected for analysis, including 11 systematic reviews and meta-analyses, 7 randomized controlled trials, and 9 primary studies of other designs, covering a total of more than 1,000 participants. EMG biofeedback statistically significantly improves gait velocity (p<0.05) and upper extremity function (evidence level 1b–2a). Stabilometric systems are effective in correcting postural control (level 2a). Neurofeedback demonstrates potential for neuroplasticity modulation in patients with severe CP, albeit with a limited evidence base (level 2b–3).
Conclusion. BF systems are an effective adjunct to conventional physical therapy in CP, providing objective progress monitoring and high patient motivation. Standardization of intervention protocols and expanding access to portable BF systems for home-based use remain priority areas.
Заключение. Успешная реабилитация при СД2 напрямую зависит от навыков самоуправления у пациента. Их развитию способствуют социальная поддержка, повышение грамотности в сфере здоровья и современные цифровые технологии.
Background. The escalating prevalence of type 2 diabetes (T2D) represents a global health issue. An integral part of T2D patient management is rehabilitation, i.e., a set of measures aimed at improving quality of life and preventing complications. In recent years, rehabilitation has seen a shift from a paternalistic approach to a patient-doctor partnership. This model assumes that patients are capable of self-management during rehabilitation. Therefore, it is important to study the determinants of effective self-management.
Objective: To identify key aspects of T2D patient rehabilitation and to examine the factors that hinder or facilitate effective self-management.
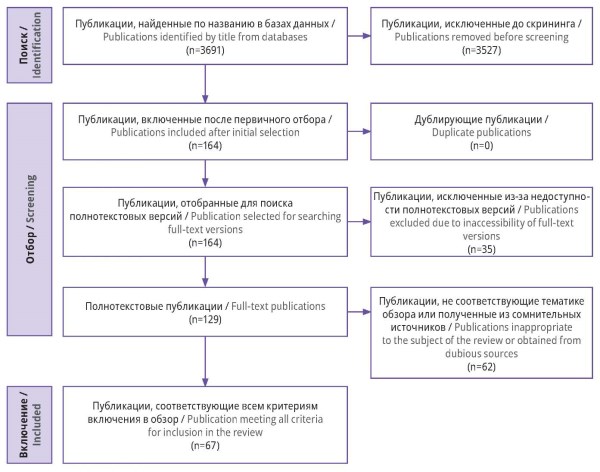
Material and methods. A literature search was conducted across scientific databases and electronic libraries: PubMed/ MEDLINE, Google Scholar, and eLibrary. A total of 3694 publications were identified, of which 70 fully met the inclusion criteria and were included in the review. The search and selection of sources were conducted in accordance with the PRISMA guidelines.
Results. The key aspects of rehabilitation in T2D patients include consistent glycemic control, dietary adjustments, regular physical activity, and proper foot care. The patient’s ability to self-manage these processes significantly impacts the effectiveness of rehabilitation. However, this is hindered by such factors as diabetes-related distress, fatigue, comorbid conditions, and lack of access to quality healthcare. Effective self-management of rehabilitation is closely linked to social support, particularly from the patient’s family. Another important factor is sufficient awareness of T2D, which allows the patient to plan the rehabilitation process effectively. Substantial support in organizing self-management is provided by modern technologies, specifically specialized mobile applications.
Conclusion. Successful management of T2D depends directly on the patient’s self-management skills. These can be developed with social support, improved health literacy, and modern digital technologies.
This study provides a review of scientific literature and regulatory documentation regarding the medical rehabilitation of patients with pulmonary tuberculosis. The integration of medical rehabilitation techniques into comprehensive care for such patients was shown to play a pivotal role in treatment optimization. This integration minimizes the risks of tuberculosisrelated complications, disability, and mortality. Furthermore, rehabilitation measures are essential for extending patients’ life expectancy and enhancing their quality of life. Noteworthy is that pulmonary tuberculosis patients require comprehensive treatment regimens that encompass both pharmacotherapy and psychological support.
СASE REPORTS

Recreational swimming is a highly effective rehabilitation method for neurological and orthopedic conditions, offering relief to the musculoskeletal system, reducing pain, and improving coordination. However, standard aquatic therapy protocols are often not applicable for patients who have undergone surgical decompression of the vertebral arteries (e.g., Kimmerle anomaly). Due to a long history of vertebrobasilar insufficiency, vestibulo-ataxic syndrome, and concomitant kinesiophobia, these patients experience high levels of anxiety and psychological barriers to aquatic activities. A clinical case of a patient who underwent two years of successful hydrotherapy after resection of the Kimmerle anomaly was analyzed. Subsequently, practical guidelines for organizing safe and effective recreational swimming were developed. These include the requirements for pool infrastructure (temperature, depth, lighting, and visual environment), special equipment (such as wetsuits, goggles, and nose clips), and the qualifications of rehabilitation trainers. Particular attention is paid to providing psychological support, following the principles of gradual adaptation, and monitoring conditions such as blood pressure and hydration. Group lessons are conducted with the support of a trained partner (buddy) to minimize fear, ensure predictability, and transform swimming from a source of stress into a tool for relaxation and socialization.
EVENTS
At the “Open Talk: The Paradigm of Rehabilitation in Women's Health” section held during the 9th Russian Congress on Physical and Rehabilitation Medicine, experts agreed that the paradigm of women's rehabilitation should fundamentally change. Rehabilitation practices for women with medical conditions related to oncology and obstetrics and gynecology need to be personalized, scientifically based, and focused on quality of life, rather than relying on traditional approaches. The International Classification of Functioning, Disabilities, and Health (ICF) is one of key tools of the new paradigm. The ICF allows for a standardized assessment of patients' physical, psycho-emotional, and social conditions, as well as the establishment of measurable goals. The resolution defines priority tasks for scientific, medical, and educational institutions, including implementing a multidisciplinary approach, developing clinical guidelines, training specialists in the use of the ICF, and establishing an expert council to further develop this direction.

ISSN 2949-5881 (Online)


