

ORIGINAL ARTICLES
Objective: To evaluate the effect of multimodal rehabilitation on anthropometric changes following radical surgery for earlystage ovarian cancer (OC).
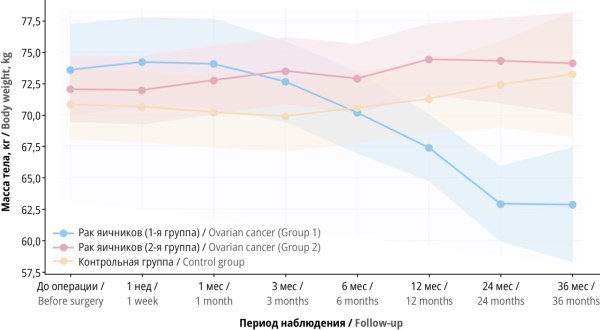
Material and methods. This prospective randomized controlled trial included 94 patients with stage I–II OC and borderline ovarian tumors, who were randomized into a multimodal “active” rehabilitation group (Group 1, n=47) and a “passive” rehabilitation group (Group 2, n=47). The control group consisted of 80 women without gynecologic malignancies. The multimo dal “active” rehabilitation program included dietary management, prescribed physical exercise, lifestyle modification, nutritional and pharmacological support. Body weight, body mass index (BMI), waist circumference, hip circumference, and waist-to-hip ratio were assessed preoperatively, as well as at 1 week; 1, 3, 6, 12, 24, and 36 months.
Results. At baseline, over 50% of patients in Groups 1 and 2 were overweight or obese. After 36 months, a significant reduction in body weight and BMI was observed in Group 1 (from 27.66±4.15 to 22.28±6.73 kg/m²; p=0.0362). The proportion of Group 1 patients with normal BMI increased from 40.4% to 71.4%. In contrast, Group 2 exhibited an increase in BMI (from 26.90±2.62 to 27.81±3.06 kg/m²; p=0.0015) and a decrease in the proportion of patients with normal BMI to 16.7%. Significant differences were also found in the waist-to-hip ratio dynamics: in Group 1, the ratio decreased from 0.89±0.05 to 0.79±0.10 (p=0.0037), indicating a shift from the “risky” to the “good” waist-to-hip ratio and reduction in abdominal obesity. In Group 2, the waist-to-hip ratio increased to 0.96±0.07.
Conclusion. The multimodal “active” rehabilitation program demonstrates high efficacy in weight correction and improvement of anthropometric parameters after early-stage OC surgery. Unlike “passive” postoperative management, which is associated with progressive weight gain and deterioration of anthropometric parameters, long-term application of this multimodal approach not only reduces body weight but also achieves a clinically significant reduction in abdominal obesity.
Objective: To justify the inclusion of input parameters in a neural network designed to predict rehabilitation measures for patients with pulmonary tuberculosis who have lost their permanent work capacity.
Material and methods. The study included 335 patients with pulmonary tuberculosis, 212 with a newly diagnosed case and 123 with a chronic form. To predict the effectiveness of rehabilitation measures, a neural network was developed in the Python 3.14 programming language. Its architecture incorporates a multilayer perceptron with direct connections between neurons and backpropagation algorithms. In the context of this study, it was advisable to use a neural network for predicting permanent disability in patients with pulmonary tuberculosis.
Results. The following were integrated as input parameters of the neural network: genotype DD of the GSTM1 gene, genotype EE of the GSTT1 gene, genotype ТС of the АВСВ1 gene and polymorphic variants of cytokine genes, including tumor necrosis factor alpha (–308G>A (rs1800629)), interleukin (IL) 1-beta (–31C>T (rs1143627)), IL-4 (–589C>T) (rs2243250)), IL-10 (–592C>A (rs1800872)), and IL-10 (–1082A>G (rs1800896)). Additionally, an adverse recurrent course, multiple and extensive drug resistance, and persistent respiratory and cardiopulmonary failure following a course of rehabilitation were incorporated. Regression analysis showed the statistical significance of all input parameters with respect to the modeling of the dependent variable. As a result of testing the neural network, the prediction accuracy (rehabilitation efficiency) was 88,3%.
Conclusion. The use of a neural network provides highly accurate predictions regarding the effectiveness of rehabilitation of patients with pulmonary tuberculosis. This method can be incorporated into clinical pulmonology practice to evaluate persistent disability in such patients. The presented predictive model is expected to form the basis of a comprehensive rehabilitation program that addresses medical, professional and social aspects.
REVIEW ARTICLES
Background. Ischemic stroke remains a leading cause of adult disability. Effective rehabilitation requires standardized outcome assessment. The lack of consensus on a set of objective indicators complicates data interpretation and clinical guideline development.
Objective: To systematically analyze objective methods for monitoring the effectiveness of rehabilitation in ischemic stroke patients and to assess their validity, reproducibility, and practical applicability.
Material and methods. A systematic search was conducted in accordance with PRISMA 2020 guidelines. International (PubMed/MEDLINE, Scopus, Web of Science, Cochrane Library, IEEE Xplore) and Russian (eLibrary and CyberLeninka) databases were searched from January 2000 to December 2024 (last search: December 15, 2024). The analysis included studies of adult ischemic stroke patients undergoing rehabilitation with objective outcome assessment. Clinical-functional scales, instrumental biomechanical methods, neuroimaging and neurophysiological markers, biochemical biomarkers, and digital assessment methods were analyzed. The risk of bias was evaluated using RoB 2, ROBINS-I, and QUADAS-2 tools.
Results. The analysis of key systematic reviews, consensus documents, and representative primary studies yielded six cate gories of objective monitoring methods. Standardized clinical-functional scales (Fugl–Meyer Assessment, National Institutes of Health Stroke Scale, Barthel Index, Functional Independence Measure, Action Research Arm Test, and Berg Balance Scale) provide the most validated basis for monitoring rehabilitation effectiveness (quality of evidence: moderate-to-high). Instrumental biomechanical methods ensure high sensitivity to changes in movement quality; however, they are characterized by high protocol variability (quality of evidence: low-to-moderate). Neuroimaging, neurophysiological, and biochemical biomarkers show significant prognostic potential but remain primarily research tools (quality of evidence: low-to-moderate). Telerehabilitation and digital assessment methods enable objective monitoring in outpatient settings (quality of evidence: low).
Conclusion. The optimal approach to monitoring rehabilitation effectiveness in ischemic stroke patients involves using a standardized set of clinical outcomes as a mandatory minimum, with gradual addition of instrumental, neurophysiological, and biomarker methods. Further development of approaches to standardizing objective rehabilitation outcomes in such patients is needed.
Total hip arthroplasty (hip replacement) is often the only option for restoring mobility in patients with osteoarthritis, rheumatoid arthritis, osteoporosis, or a proximal femur fracture. Demand for such surgeries is increasing every year; however, the number of postoperative complications associated with them is also growing. Many of these complications – deep vein thrombosis, dislocation, and loosening of the prosthesis – arise due to insufficient attention to rehabilitation measures during the pre- and postoperative phases. Therefore, adherence to the comprehensive protocol of therapeutic and rehabilitative measures is essential when aiming to optimally restore joint function and enable patients to resume their usual physical activities. This study reviews the main stages of rehabilitation for patients following hip replacement surgery. These stages include preoperative rehabilitation, pain management, and early postoperative rehabilitation in an inpatient setting. An outpatient rehabilitation protocol focusing on gait biomechanics correction is also discussed. Comprehensive rehabilitation plays a crucial role in improving quality of life after hip replacement surgery.
Advances in medical science and healthcare significantly reduce the risk of severe liver disease progression in patients with metabolic disorders. Currently, non-alcoholic fatty liver disease (NAFLD) represents a global challenge for hepatology and rehabilitation medicine, with therapeutic exercise serving as the most effective non-pharmacological method to achieve steatosis regression and improve the metabolic profile. This literature review provides a systematic effectiveness analysis of various physical activity regimens in the management of NAFLD patients, which encompasses prevention, treatment, and rehabilitation. Molecular and biomechanical mechanisms of exercise, modern techniques for prescribing aerobic and resistance loads, and clinical applications of therapeutic exercise are discussed. Special attention is paid to the evidence base from randomized controlled trials and meta-analyses.
Over five years have passed since the COVID-19 outbreak, but the rehabilitation of coronavirus patients still remains a highly relevant issue. In the search for new rehabilitation approaches, researchers have turned their attention to intermittent hypoxic-hyperoxic therapy (IHHT) as a means of restoring impaired physical and psychological body reserves. IHHT promotes comprehensive recovery by modulating metabolic and immune processes as well as antioxidant defenses. Numerous clinical studies indicate the potential of this rehabilitation modality, which is supported by its efficacy, safety, and the preservation of achieved effects for three to six months. The reviewed publications report the IHHT effectiveness in patients with combined pathology. However, a number of identified limitations currently prevents this method from being scaled up to the level of standard rehabilitation protocols, which, together with the existing body of evidence, raises the need for a large multicenter study to evaluate the efficacy and safety of IHHT in patients with post‑COVID syndrome of varying severity.
Traditional rehabilitation methods are often limited by patient compliance issues and deficiencies in objective feedback, which are necessary for significant functional improvement. Therefore, new approaches should be implemented to improve patient motivation and increase therapy effectiveness. The increasing use of virtual reality (VR) and augmented reality (AR) technologies in rehabilitation is a solution. While VR creates a fully immersive digital environment that replaces the real world and requires the use of headsets, AR overlays digital elements onto the real world: using smart glasses, tablets, or VR headsets, patients can see both their physical surroundings and virtual cues. Thus, these technologies provide real-time feedback and cues during exercise. This study reveals the effectiveness of VR and AR technologies for rehabilitating patients with functional impairments resulting from cancer, stroke, multiple sclerosis, traumatic brain injury, low vision, and musculoskeletal disorders. These techniques relieve pain while improving function, mental health, and quality of life. High patient compliance with these rehabilitation methods has been demonstrated. The reasons for the success of these technologies are discussed, as well as the challenges hindering their widespread implementation in clinical practice.

ISSN 2949-5881 (Online)


